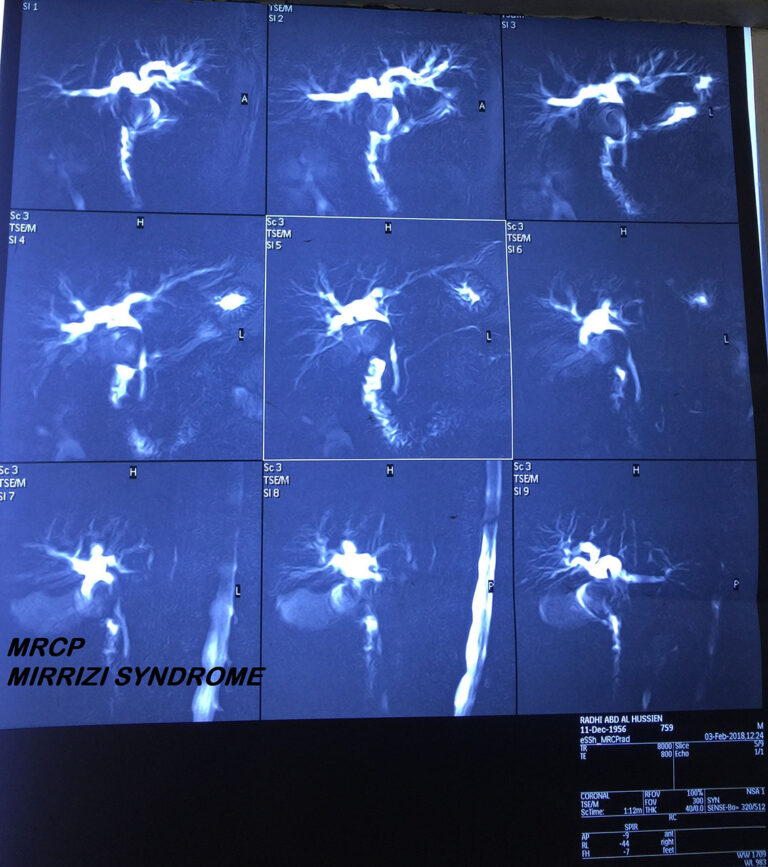
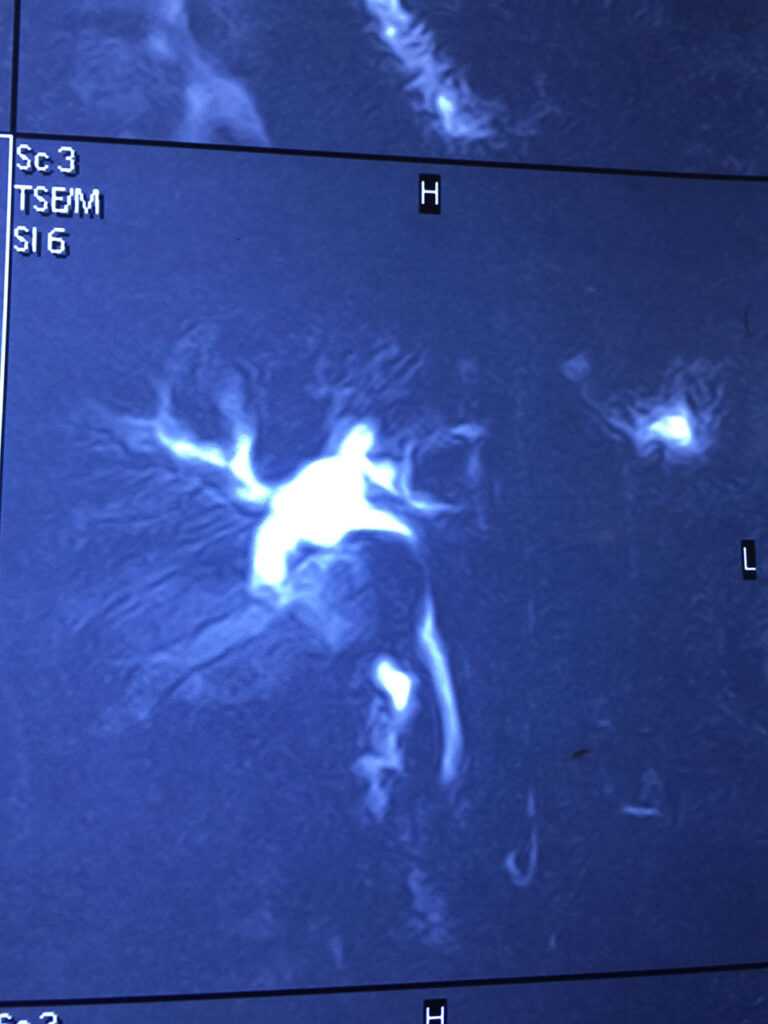
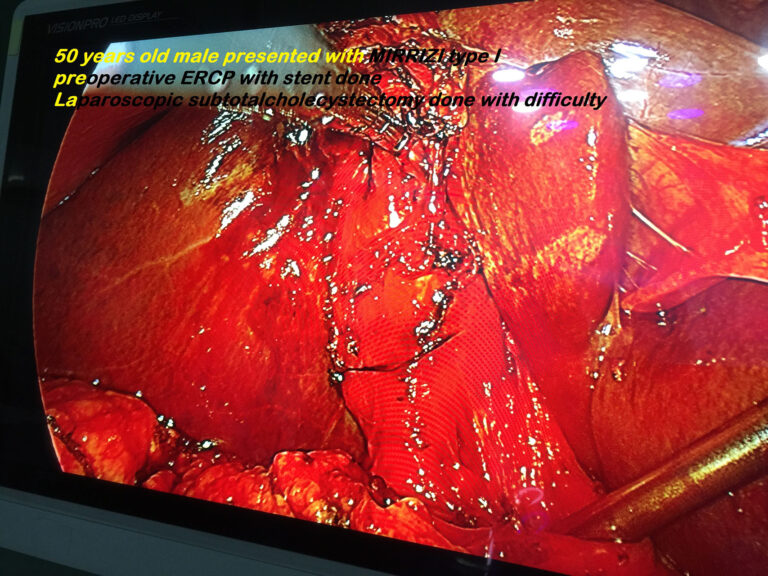
Mirrizi type I Difficult Laparoscopic Cholecystectomy (June 2018)
Review Of Literature
World J Gastroenterol. 2012 Sep 14; 18(34): 4639–4650. Published online 2012 Sep 14. doi: 10.3748/wjg.v18.i34.4639 PMCID: PMC3442202 PMID: 23002333 Mirizzi syndrome: History, current knowledge and proposal of a simplified classification Marcelo A Beltrán
Abstract
Chronic complications of symptomatic gallstone disease, such as Mirizzi syndrome, are rare in Western developed countries with an incidence of less than 1% a year. The importance and implications of this condition are related to their associated and potentially serious surgical complications such as bile duct injury, and to its modern management when encountered during laparoscopic cholecystectomy. The pathophysiological process leading to the subtypes of Mirizzi syndrome has been explained by means of a pressure ulcer caused by an impacted gallstone at the gallbladder infundibulum, leading to an inflammatory response causing first external obstruction of the bile duct, and eventually eroding into the bile duct and evolving to a cholecystocholedochal or cholecystohepatic fistula. This article reviews the life of Pablo Luis Mirizzi, describes the earlier and later descriptions of Mirizzi syndrome, discusses the pathophysiological process leading to the development of these uncommon fistulas, reviews the current diagnostic modalities and surgical approaches and finally proposes a simplified classification for Mirizzi syndrome intended to standardize the reports on this condition and to eventually develop a consensual surgical approach to this unexpected and seriously dangerous condition.
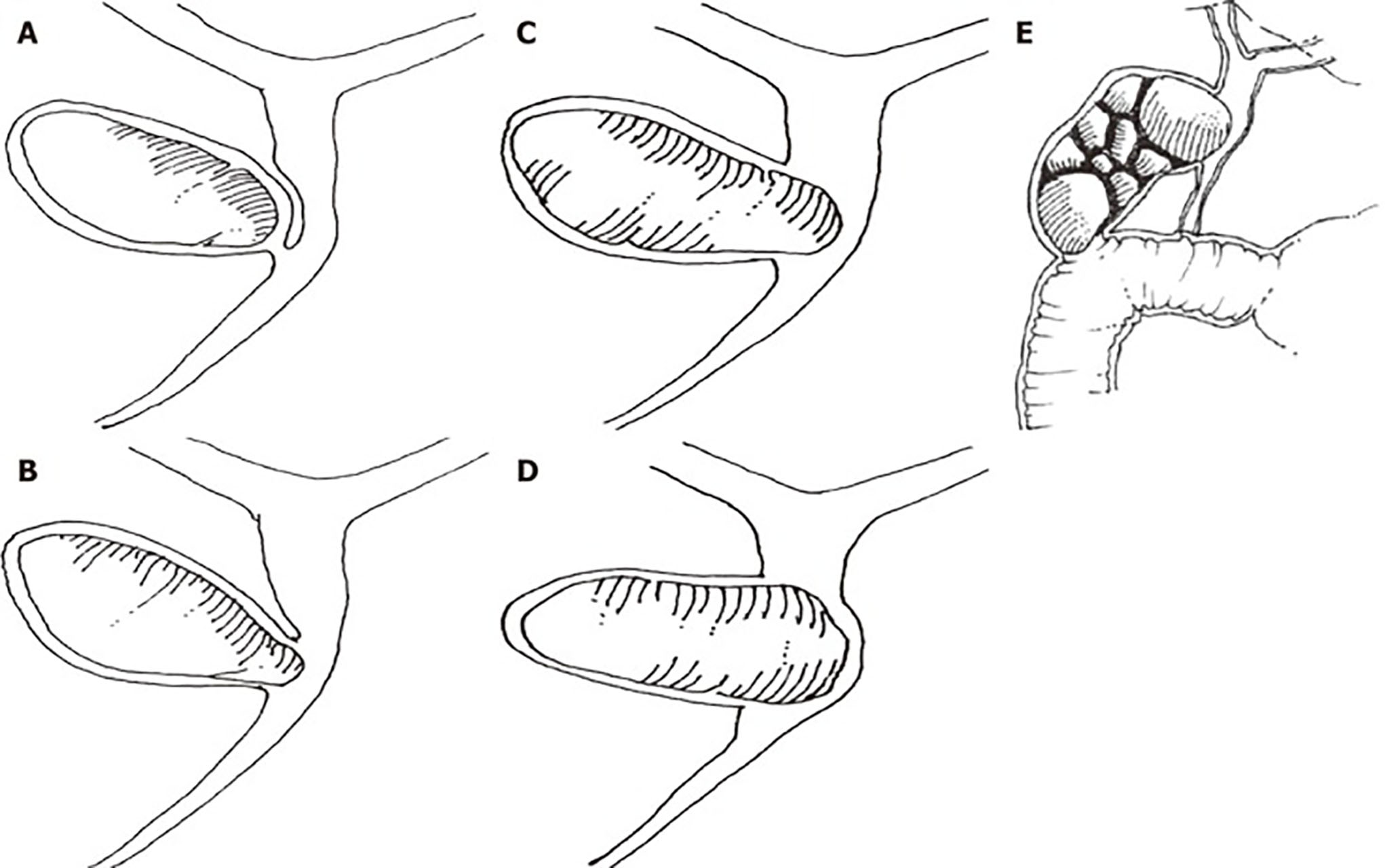
A: Mirizzi type I is the extrinsic compression of the common bile duct by an impacted gallstone; B: Mirizzi type II consists of a cholecystobiliary fistula involving one third of the circumference of the bile duct; C: In Mirizzi type III, the cholecystobiliary fistula compromises up to two-thirds of the circumference of the bile duct; D: In Mirizzi type IV, the cholecystobiliary fistula has destroyed the bile duct wall, and comprises the whole circumference of the bile duct; E: Mirizzi type V corresponds to any type of Mirizzi associated with a bilioenteric fistula with or without gallstone ileus.
(original drawings from World Journal of Surgery 2008; 32, pages 2239 to 2241)[4].
Related Cases
CONCOMITANT TOTAL THYROIDECTOMY AND RIGHT TOTAL MASTECTOMY PLUS AXILLARY LYMPH…
CONCOMITANT TOTAL THYROIDECTOMY AND LEFT PAROTIDECTOMY IN 69 YEAR OLD…
LEFT TOTAL PAROTIDECTOMY FOR RECURRENT PAROTID MASS (OCT.2022)
Right submandibular salivary gland excision (Sep.2022)