Choleduchocele (Type 3B choleduchal cyst) masquerading as Duodenal duplication cyst (June 2019)
Case presentation
A 3-year-old boy was admitted to the hospital for acute abdominal pain associated with vomiting and fever. Although his symptoms disappeared quickly with anti-infectious therapy, he had repeated episodes of abdominal pain frequently in the following 6 months; the pain lasted for several minutes and alleviated spontaneously. At that time, he showed no other symptoms, and his physical examination and serum chemistry levels were normal.
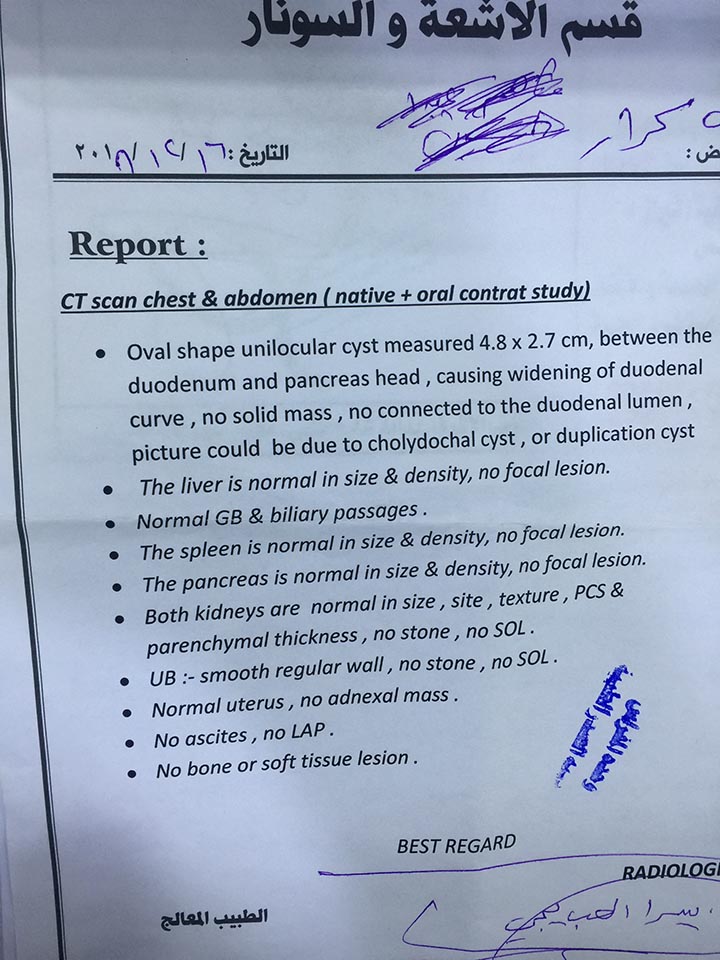
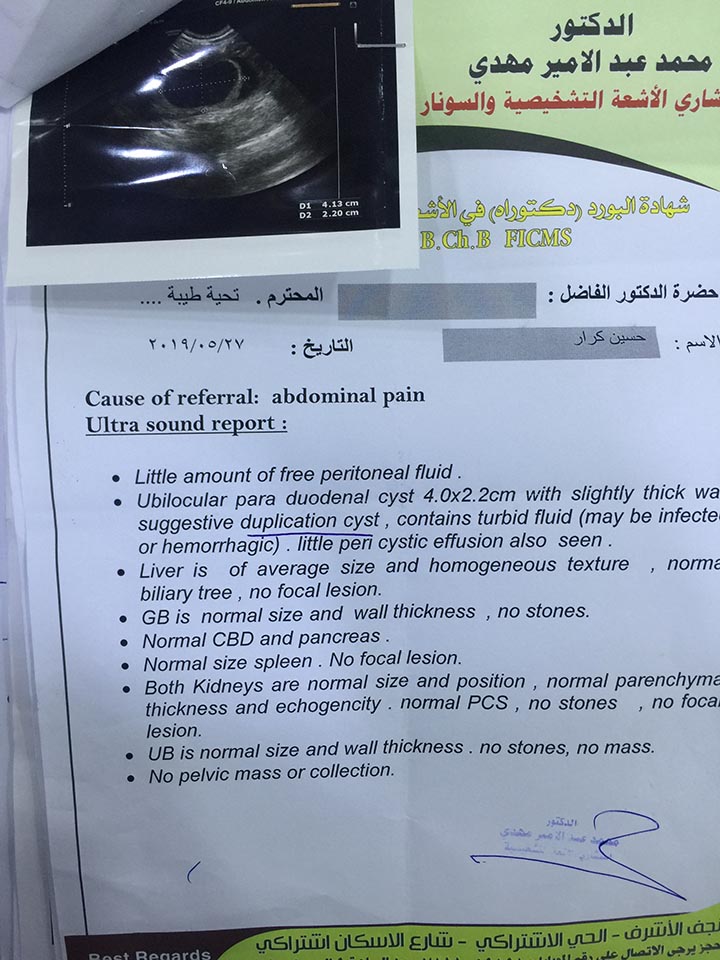
At first admission the ultrasound examination revealed paradoudenal cyst most probably duplication cyst; confirmed by CT scan of abdomen. There was no other significant medical history, and the family history was not pertinent.
The patient put on conservative treatment and postpond surgical intervention because his parents refused surgery.
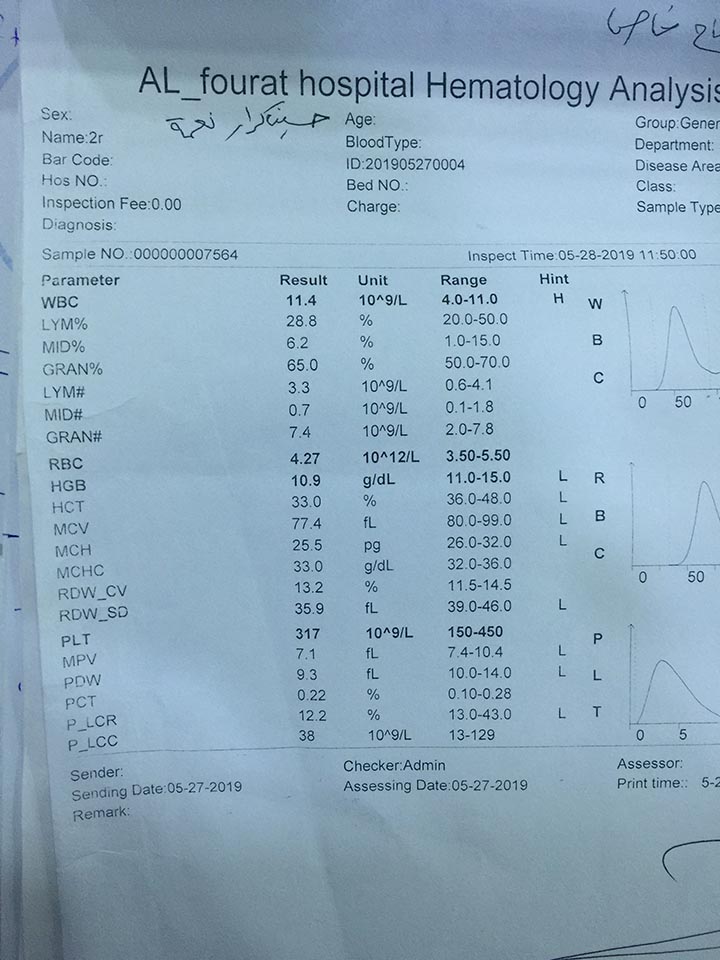
The child was admitted, and the investigations obtained at our hospital were as follow
Liver function tests were normal. Ultrasound examination revealed a paradoudenal cyst (4 cm × 2.6 cm ) on the right of the head of the pancreas .
On upper gastrointestinal X-ray barium meal, NO filling defect was noted on the duodenal parts .
Endoscopic gastroduodenoscopy was NOT done.
A provisional diagnosis of duodenal duplication was made and planned for surgery at same admission.
Case presentation
Clin Gastroenterol Hepatol. 2014 Feb;12(2):196-203. doi: 10.1016/j.cgh.2013.04.037. Epub 2013 May 6.
Diagnosis and treatment of choledochoceles.
Law R1, Topazian M2.
Author information
Abstract
Choledochoceles are cystic dilatations of the intraduodenal portion of the common bile duct. Although often classified as Type III biliary cysts, choledochoceles have distinctive demographic and anatomic features and a lower risk of malignancy than other types of choledochal cysts. Type A choledochoceles are cystic dilatations of a segment of the intra-ampullary bile duct and are located proximal to the ampullary orifice. Type B choledochoceles are diverticula of the intra-ampullary common channel and are located distal to the ampullary orifice; they can be distinguished from duodenal duplication cysts both anatomically and histologically. Both types of choledochocele may present with pancreatitis, biliary obstruction, or nonspecific gastrointestinal symptoms. Cross-sectional imaging, endoscopic ultrasound, and endoscopic retrograde cholangiopancreatography are useful for diagnosis. Choledochoceles may be drained or resected endoscopically. Surveillance for dysplasia should be considered for lesions that are not resected.Copyright © 2014 AGA Institute. Published by Elsevier Inc. All rights reserved.
KEYWORDS:
CBD; CT; Choledochal Cyst; ERCP; EUS; MRCP; MRI; Sphincterotomy; US; common bile duct; computed tomography; endoscopic retrograde cholangiopancreatography; endoscopic ultrasound; magnetic resonance cholangiopancreatography; magnetic resonance imaging; ultrasoundEuropean J Pediatr Surg Rep. 2015 Dec; 3(2): 85–89.
Published online 2015 Sep 9. doi: 10.1055/s-0035-1563601
PMCID: PMC4712052
PMID: 26788455
Choledochocele: A Case Report and Discussion of Diagnosis Criteria
Linlin Zhu,1 Zhibao Lv,1 Jiangbin Liu,1 and Weijue Xu1
Author information Article notes Copyright and License information Disclaimer
Abstract
A 6-year-old girl presented with intermittent abdominal pain, without jaundice and a palpable mass in the epigastrium. Preoperative imaging and upper endoscopy suggested duodenal duplication. During surgery, the patient was diagnosed with a rare type of choledochal cyst—choledochocele (type 3b). The authors emphasize that, in children, choledochocele should be included in the differential diagnosis of cystic lesions located in the duodenal area and the head of the pancreas area, regardless of jaundice or abnormal liver function. Since mucosal histology showing duodenal mucosa did not match the final diagnosis, we suggest that three criteria should be met for the diagnosis of a choledochocele to be diagnosed: (1) a cyst protruding into the duodenal lumen; (2) filling with contrast during cholangiography and (3) a filling defect on X-ray barium meal.Keywords: choledochocele, duodenal duplication, radiologic criteria