RIEDLE’S LOBE ENCOUNTERED DURING FUNDUS FIRST LAPAROSCOPIC CHOLECYSTECTOMY (SEP. 2021)
Case summary
A 42-year-old man with a history of known gallstone disease presented to the office with worsening post-prandial right upper abdominal pain radiating to the back, abdominal bloating, and nausea. His clinical history was significant for hypertension and hyperlipidemia. His vitals were within normal limits, and physical examination showed right upper quadrant tenderness with positive Murphy’s sign. Laboratory studies including complete blood cell count, and coagulation panel were within normal limits. Liver function tests were mildly elevated. An ultrasound of the abdomen confirmed the diagnosis of acute cholecystitis. There was no indication of an accessory lobe AL on the ultrasound images. After a 6 weeks of conservative management of acute cholecystitis , a decision was made to proceed with an elective laparoscopic cholecystectomy.
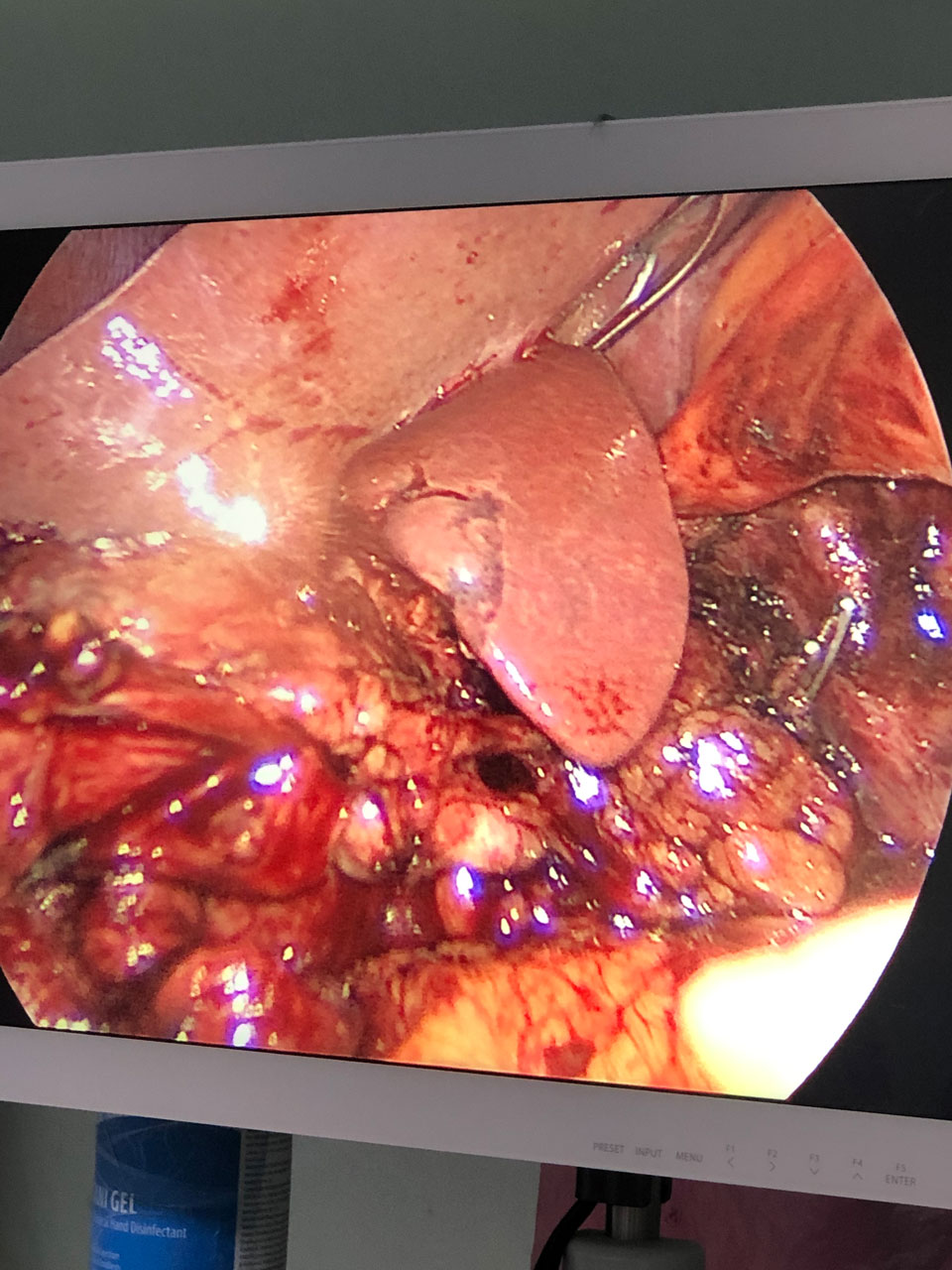
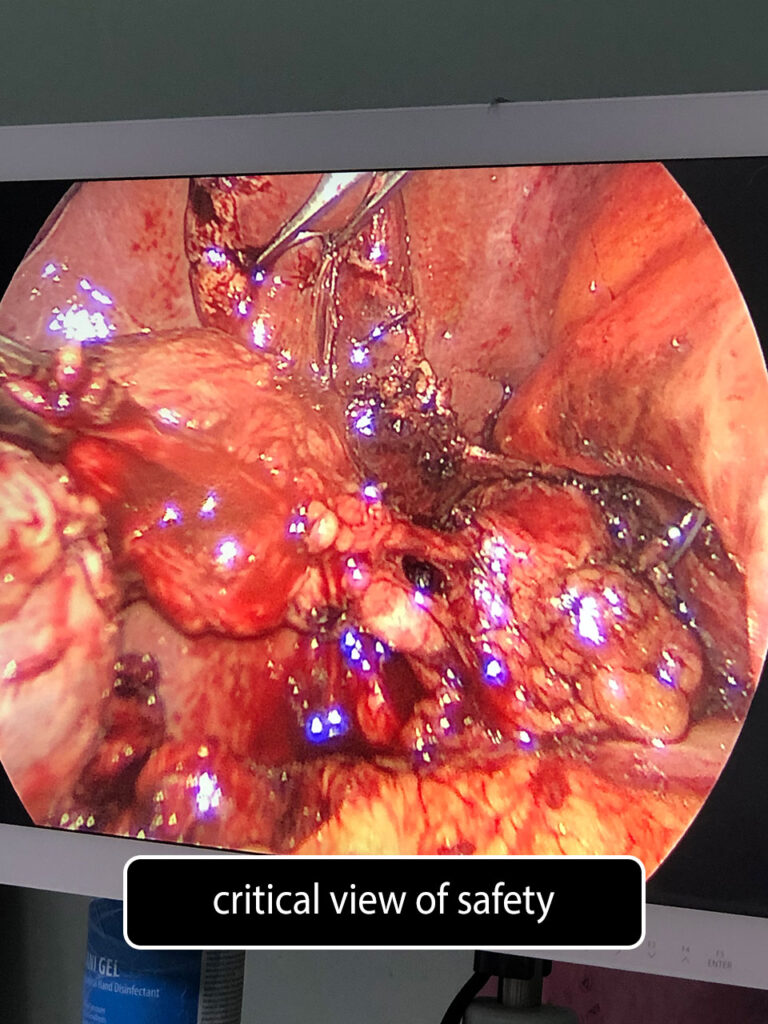
This finding was consistent with the diagnosis of an AL with its attachment to the gallbladder. After achieving the critical view of safety, the cystic duct and cystic artery were secured with laparoscopic endoclips and transected. The GB was dissected from AL which representing liver bed.
The patient tolerated and recovered from the procedure well, and he was discharged to home on the day of surgery without complications.
Review of literature
An accessory liver lobe (AL) or (Riedle’s lobe RL) is a rare congenital anomaly generally due to either defective or excessive development of the liver [1]. It was first described as a lobe of the liver connected to the main liver via a dense membrane by Morgagni in 1767 [2]. Although it can rarely cause abdominal pain and liver dysfunction, RL mostly remains asymptomatic and is commonly found incidentally during laparotomy, autopsy, and radiologic studies [1].
We report a case of an ectopic AL that was incidentally found to be attached to the posterior surface of the gallbladder wall forming GB bed during laparoscopic cholecystectomy.
References
Complete hepatic ischemia due to torsion of a large accessory liver lobe: first case to require transplantation. Ladurner R, Brandacher G, Mark W, et al. Transpl Int. 2005;18:467–469.
De sedibus et causis morborum. Epistolae II. 1767;48:55