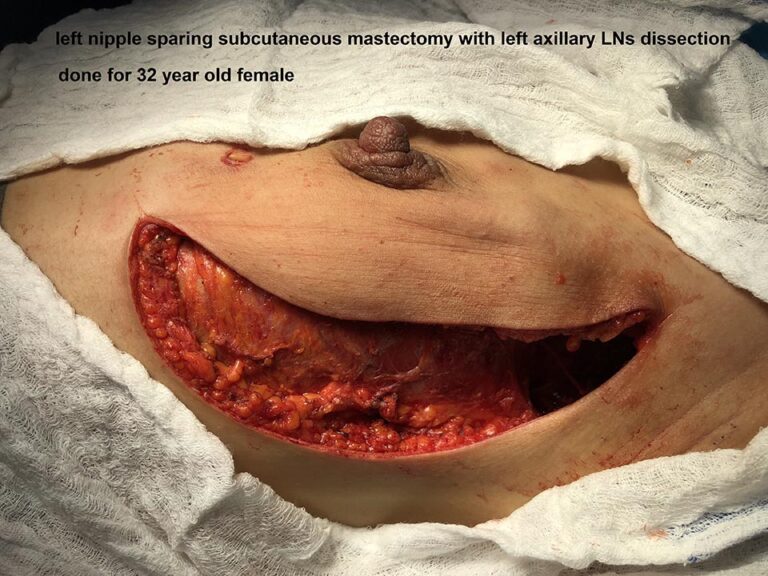
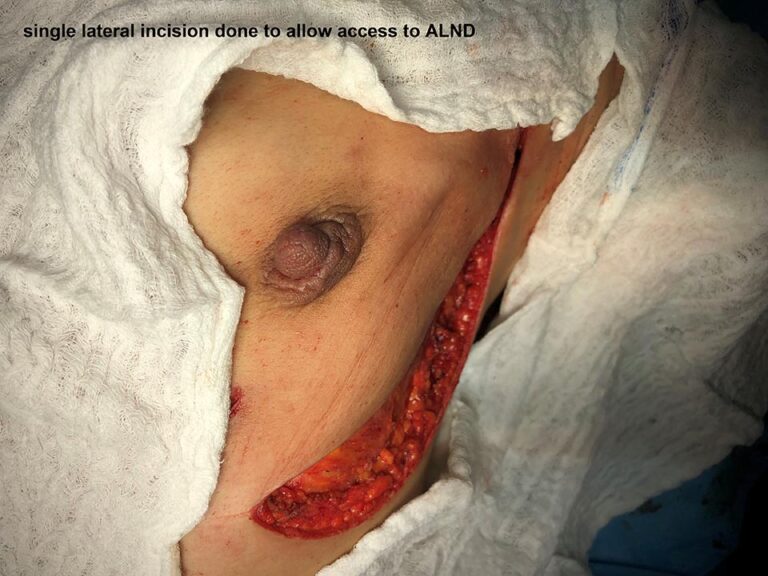
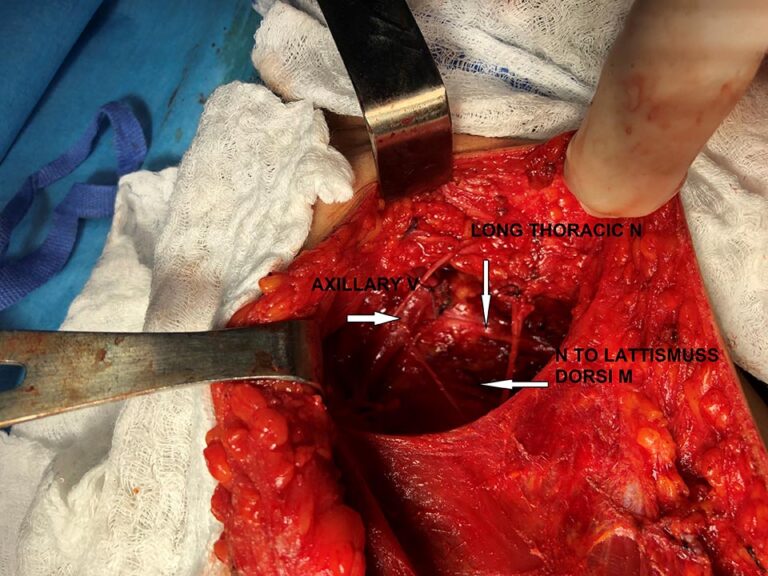
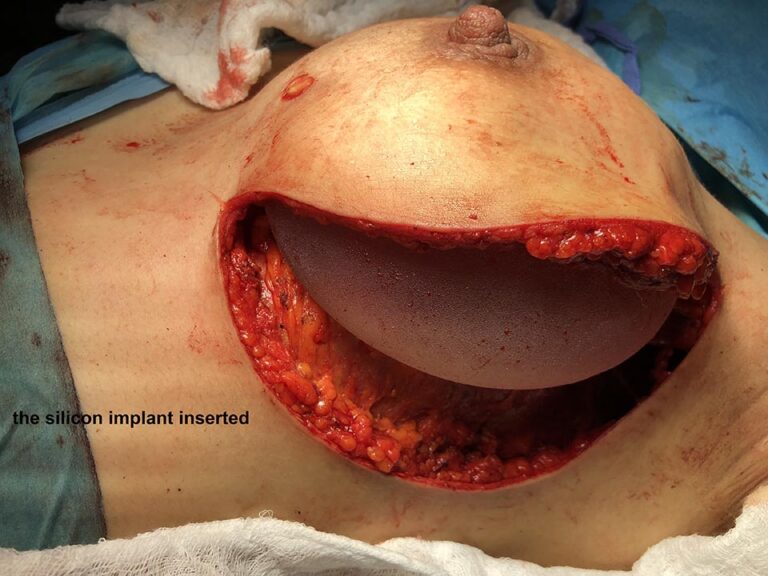
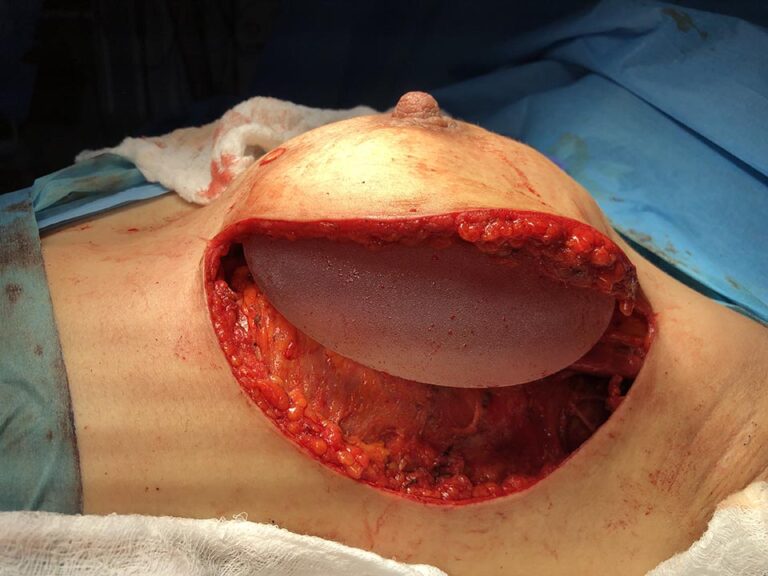
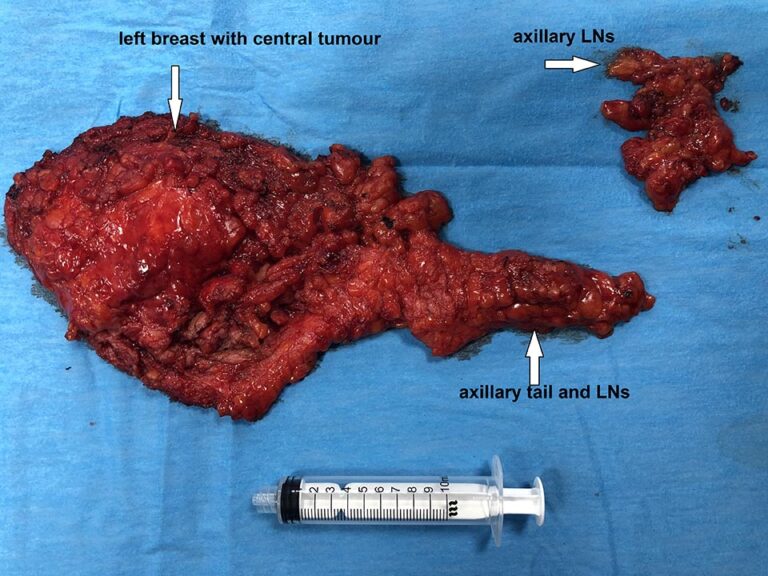
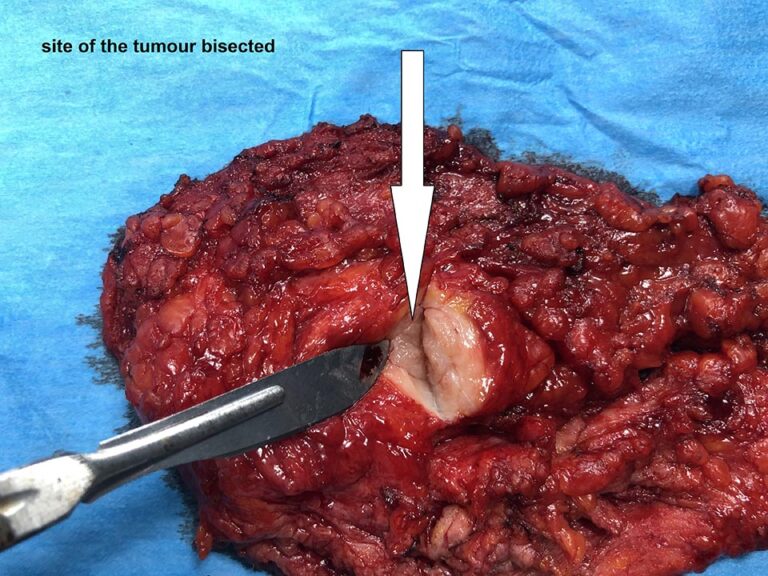
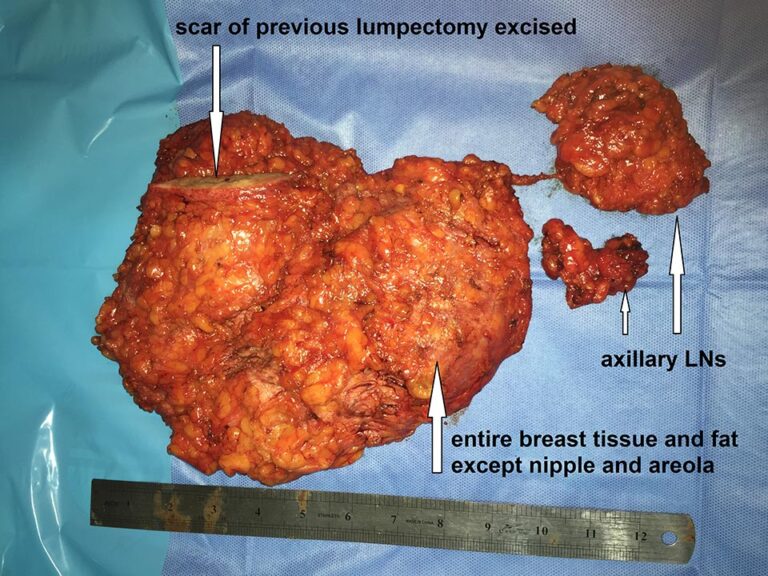
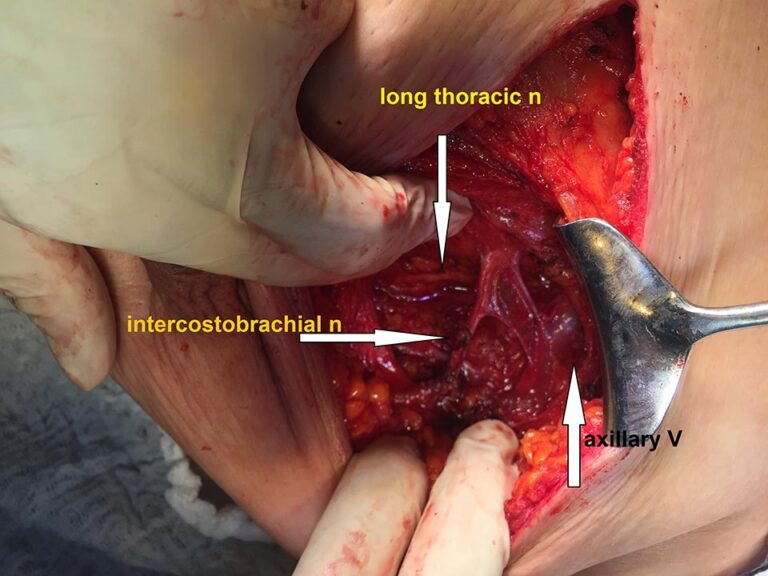
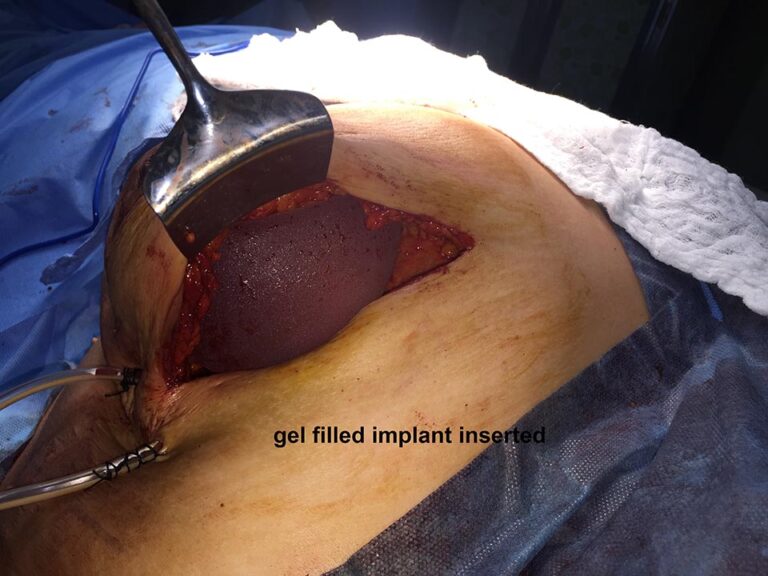
Nipple Sparing Mastectomy with Primary Implant plus axiliary dissection (Sep. 2019)
Case 1
Case 2
Review of literature
Nipple-Sparing Mastectomy and Direct-to-Implant Breast Reconstruction. Colwell AS1, Christensen JM. Author information 1 Boston, Mass. From the Division of Plastic and Reconstructive Surgery, Massachusetts General Hospital, Harvard Medical School.
Abstract
Breast reconstruction following mastectomy has evolved to preserve the native skin and nipple of the breast and create a natural-appearing reconstruction in 1 or 2 surgeries. Nipple-sparing procedures appear to be oncologically safe with low risks of cancer recurrence. In our series of 2,182 nipple-sparing mastectomies, there was no development or recurrence of cancer in the nipple. Direct-to-implant single-stage surgery offers the patient a complete reconstruction at the time of mastectomy. Patient selection centers on preoperative breast anatomy combined with postoperative goals for size and uplift of the breast. The best candidates for nipple-sparing mastectomy and direct-to-implant breast reconstruction include those with grade I-II breast ptosis and those desiring to stay approximately the same breast size. The choice of incision and width of the implant play key roles in nipple centralization. Partial muscle coverage with acellular dermal matrix remains the most common technique to support the implant and offers the advantage of more soft-tissue coverage in the upper pole. With experience, complications and revisions are similar in this approach compared with more traditional 2-stage tissue expander-implant reconstruction. Thus, nipple-sparing mastectomy and direct-to-implant breast reconstruction is emerging as a preferred method of breast reconstruction when the breast skin envelope is sufficiently perfused.
Related Cases
CONCOMITANT TOTAL THYROIDECTOMY AND RIGHT TOTAL MASTECTOMY PLUS AXILLARY LYMPH…
CONCOMITANT TOTAL THYROIDECTOMY AND LEFT PAROTIDECTOMY IN 69 YEAR OLD…
LEFT TOTAL PAROTIDECTOMY FOR RECURRENT PAROTID MASS (OCT.2022)
Right submandibular salivary gland excision (Sep.2022)