Solid Pancreatic Pseudopapillary Tumor Managed Laparoscopically (May 2018)
Case presentation
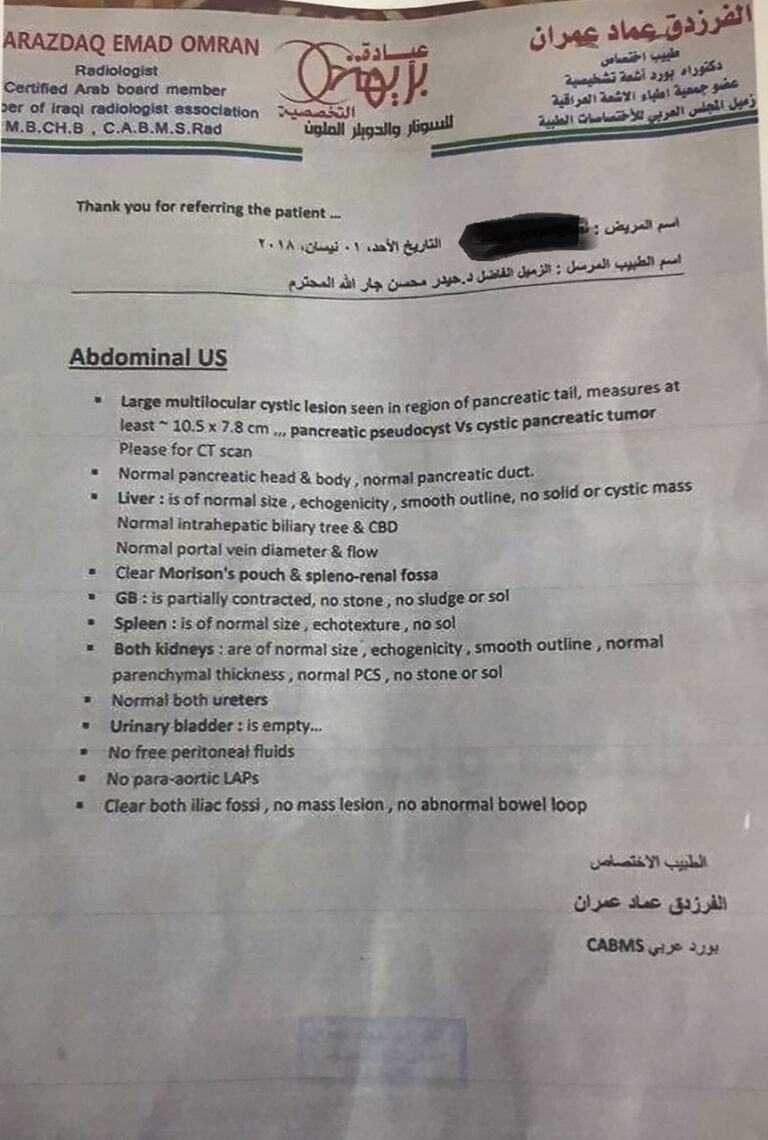
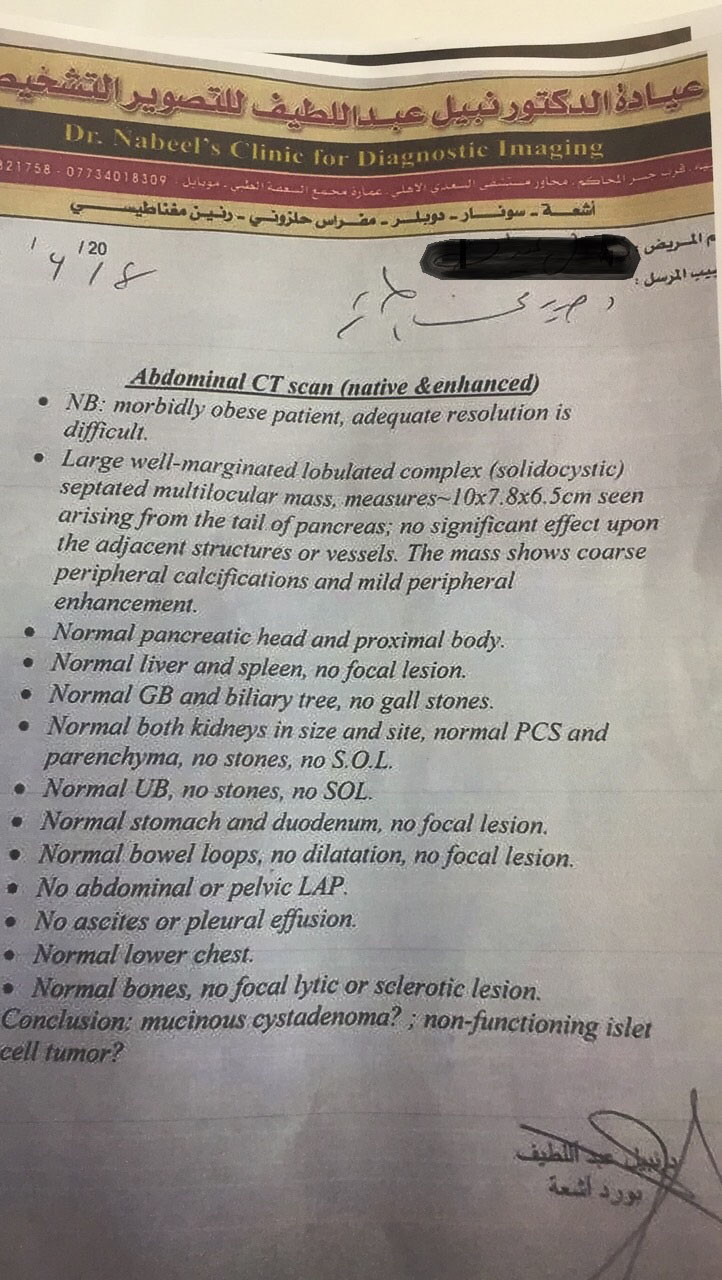
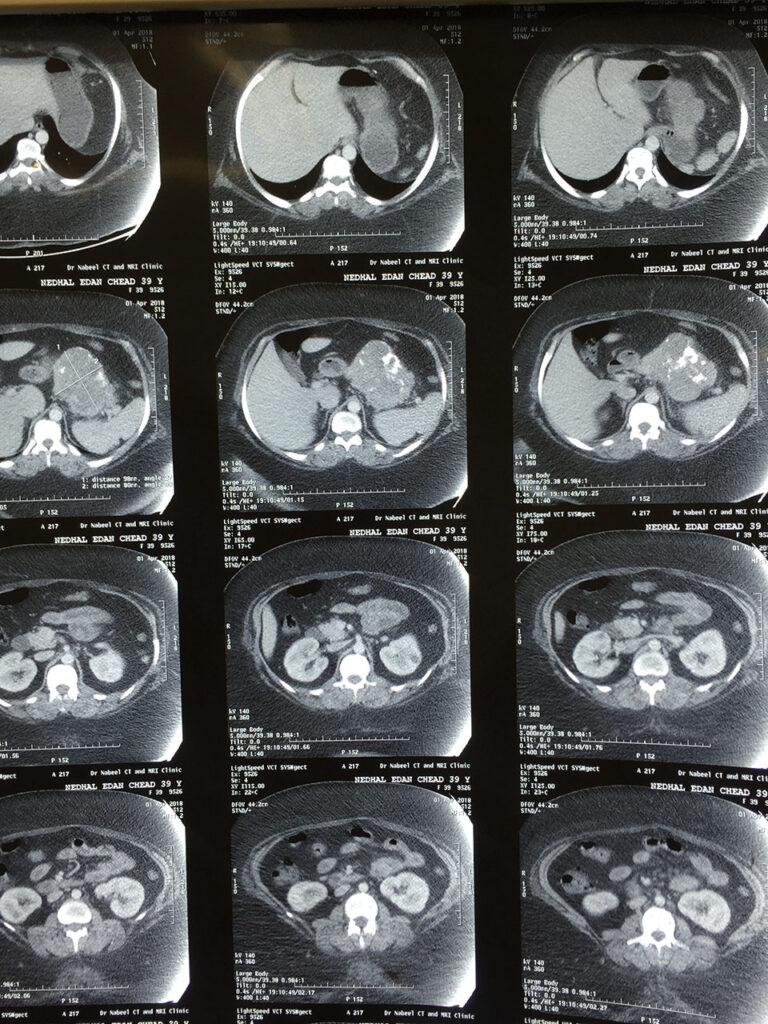
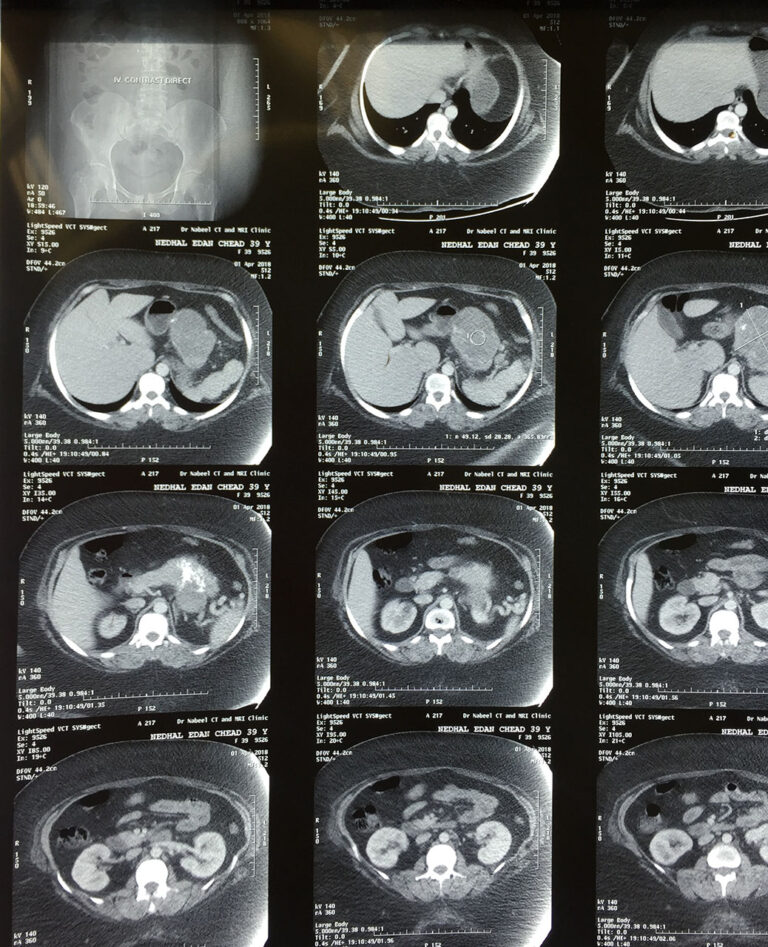
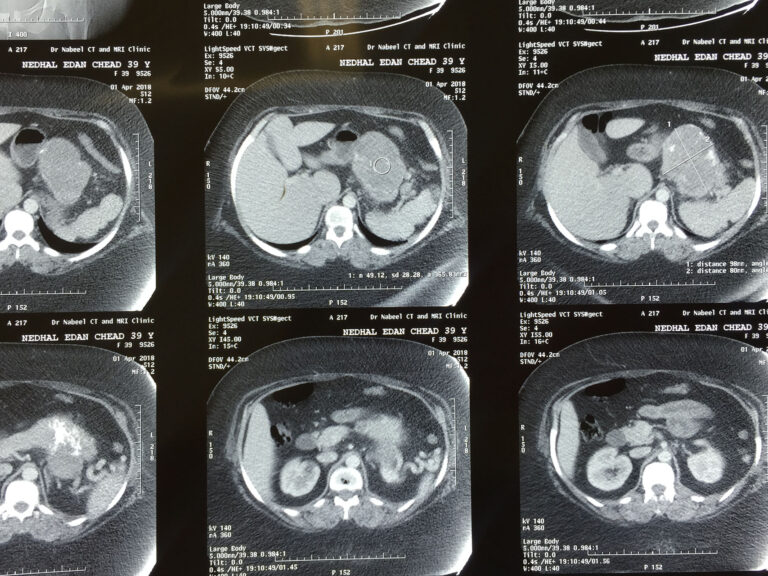
41 years old morbidly obese female patient presented with upper abdominal pain for one month duration. Abdominal ultrasound and CT scan revealed large distal pancreatic complex (solid and cystic) 10 * 8 cm mass reaching the splenic hilum. The hematological and biochemical tests were within normal values. Tumor markers ( CEA , CA 19-9, CA 125, CA 15-3 ) were NEGATIVE. There was no comorbidity.
Preparation for laparoscopic surgery was done and thromboprophylaxis measures were achieved.
Under general anesthesia and head up French position, 5 ports inserted : 2 ports of 12 mm ,one port of 10 mm , and 2 ports of 5mm.
LigaSure sealing device was used. Gastro colic omentum opened and lesser sac entered.
Dissection proceeded along upper border of large distal pancreatic mass about 10 – 12 cm in diameter, then lower border dissected and the 2 planes met posterior to pancreas (disease free area) and identification with separation of both splenic artery and vein was done. The pancreatic body encircled by nylon tape prepared for transaction.
60 mm Covideon linear laparoscopic violet stapler used for transaction. The splenic vessels clipped (by haem O lock) and divided. The dissection of the mass continued toward splenic hilum and splenectomy completed after division of short gastric vessels and adhesions with diaphragm.
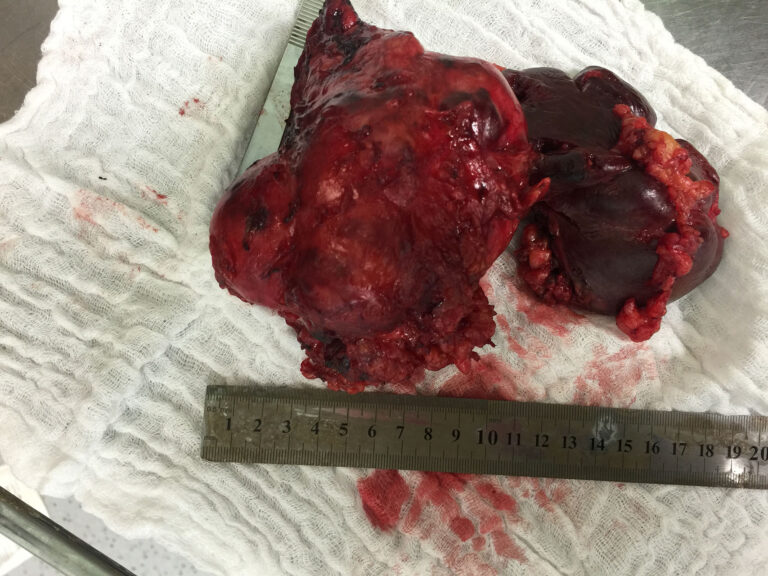
So spleno distal pancreasectomy was completed.
Minilaparotomy incision in the midline done to extract the mass and spleen. Tube drain put in the left side of abdomen and abdominal incision closed in layers by nylon suture. The operative time was 5 hours. The recovery was smooth and uneventful postoperative course.
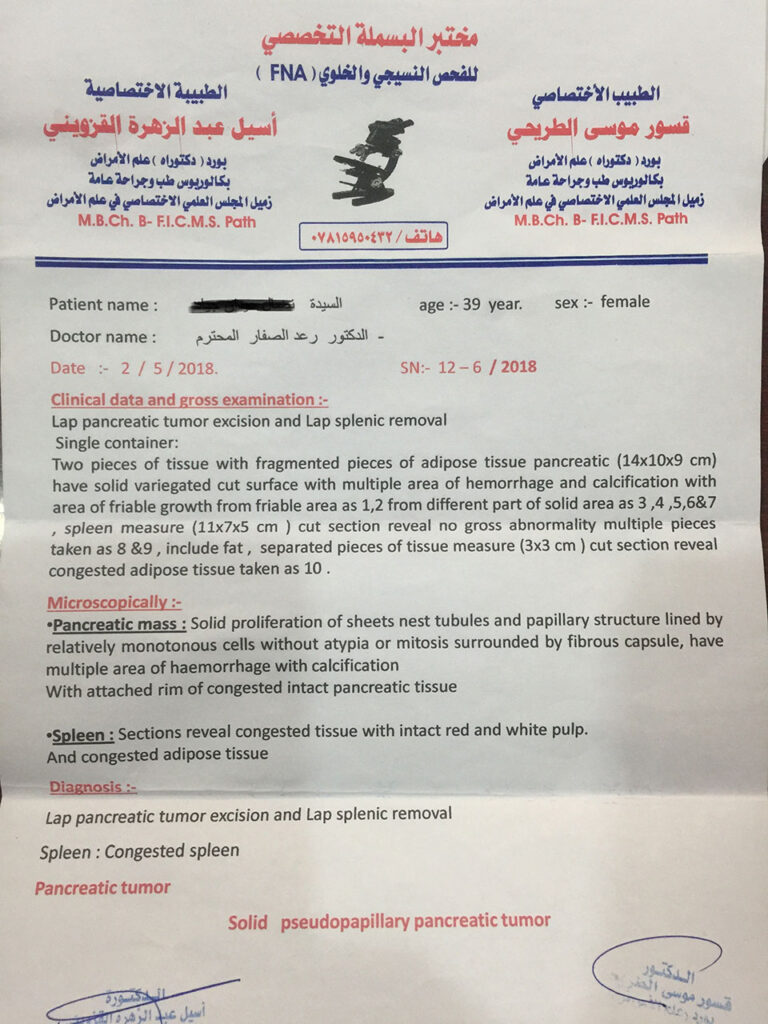
The histopathological report was solid pancreatic pseudopapillary tumor.





REVIEW OF LITERATURE
Case Report
Solid pancreatic pseudopapillary tumor managed laparoscopically: A case report and review of the literature
Author links open overlay panelD.CuccurulloaG.CarbonebM.G.IovinobI.De RosaaM.FabozziaF.Corcionea
https://doi.org/10.1016/j.ijscr.2017.12.043
Highlights
- Solid pancreatic pseudopapillary tumors are a rare neoplasms with not well known pathogenesis.
- Imaging is not able to provide a precise diagnostic orientation. The essential role is played by surgery and histological examination.
- Immunohistochemistry shows a possible correlation between the Beta-catenin mutations or alteration of the E-cadherin and tumor development.
- Laparoscopic technique has proven to be the gold standard for the countless advantages found compared to the open technique.
Abstract
Background
Solid pancreatic pseudopapillary tumors are a rare neoplasms, about 1–3% of all pancreatic neoplasms. This cancer mainly affects women between the third and fourth decade of life.
They are not well known; the molecular origins represent a low degree of malignancy, in which the complete resection is curative. We report our experience with a case report of SPT in a young man.
Presentation of case
Thirty-six years old male patient with a mass about 10 cm in the pancreatic tail and splenic hilum. After following CT and MR, the patient was subjected to surgery. Histophatological result was solid tumor pseudopapillary of pancreas with no pathological lymph nodes.
Discussion and conclusion
Solid pseudopapillary neoplasm shows histological characteristic solid and pseudopapillary proliferation. Immunohistochemistry detects, among the causes of tumor development, a correlation between the Beta-catenin mutations, alteration of the E-cadherin. In the most cases, therapy is surgical treatment with laparoscopic.
Keywords
Pancreatic pseudopapillary neoplasm Pancreatic tumor Laparoscopic surgery.